


In July, the Centers for Medicare & Medicaid Services introduced significant changes to the Staffing Five-Star domain, impacting how staffing adjustments are made in relation to resident acuity.
Previously, these adjustments relied on the STRIVE study, which primarily used historical data to estimate the acuity of residents. However, CMS now uses the Patient-Driven Payment Model nursing case-mix index (CMI) to perform these adjustments.
This transition has caused confusion among providers and external stakeholders alike. Many are uncertain about how CMS calculates these adjustments, what role Minimum Data Set coding accuracy plays, and how payer mix influences the adjustments. Moreover, questions are being raised about whether external factors beyond resident acuity affect the new staffing adjustment formula.
Background on staffing adjustment
The staffing adjustment in the CMS Five-Star Rating system is now based on the PDPM nursing CMI. CMS’ change ensures that facilities’ staffing ratios are evaluated based on the acuity of the residents they serve, not solely on their unadjusted staffing levels. Facilities with residents requiring higher levels of care are expected to have higher staffing levels to achieve optimal outcomes.
According to the CMS Five-Star technical manual, the Staffing domain rating is adjusted to account for resident acuity. At its core, MDS coding directly influences the nursing CMI and, consequently, the staffing adjustment in the Five-Star rating system.
The accuracy of MDS coding is critical because it serves as the primary source of data for calculating CMI. Incorrect or inconsistent MDS coding can lead to a distorted CMI, which in turn can result in over- or underestimation of required staffing levels.
National analysis of nursing CMI distribution
The distribution of nursing CMI across facilities nationwide demonstrates significant variation. Some facilities have a disproportionately high nursing CMI, while others fall well below national averages. This variance can often be attributed to differences in MDS coding practices, resident acuity and the types of payers that dominate a facility’s revenue stream and location.
National Distribution of Nursing CMI

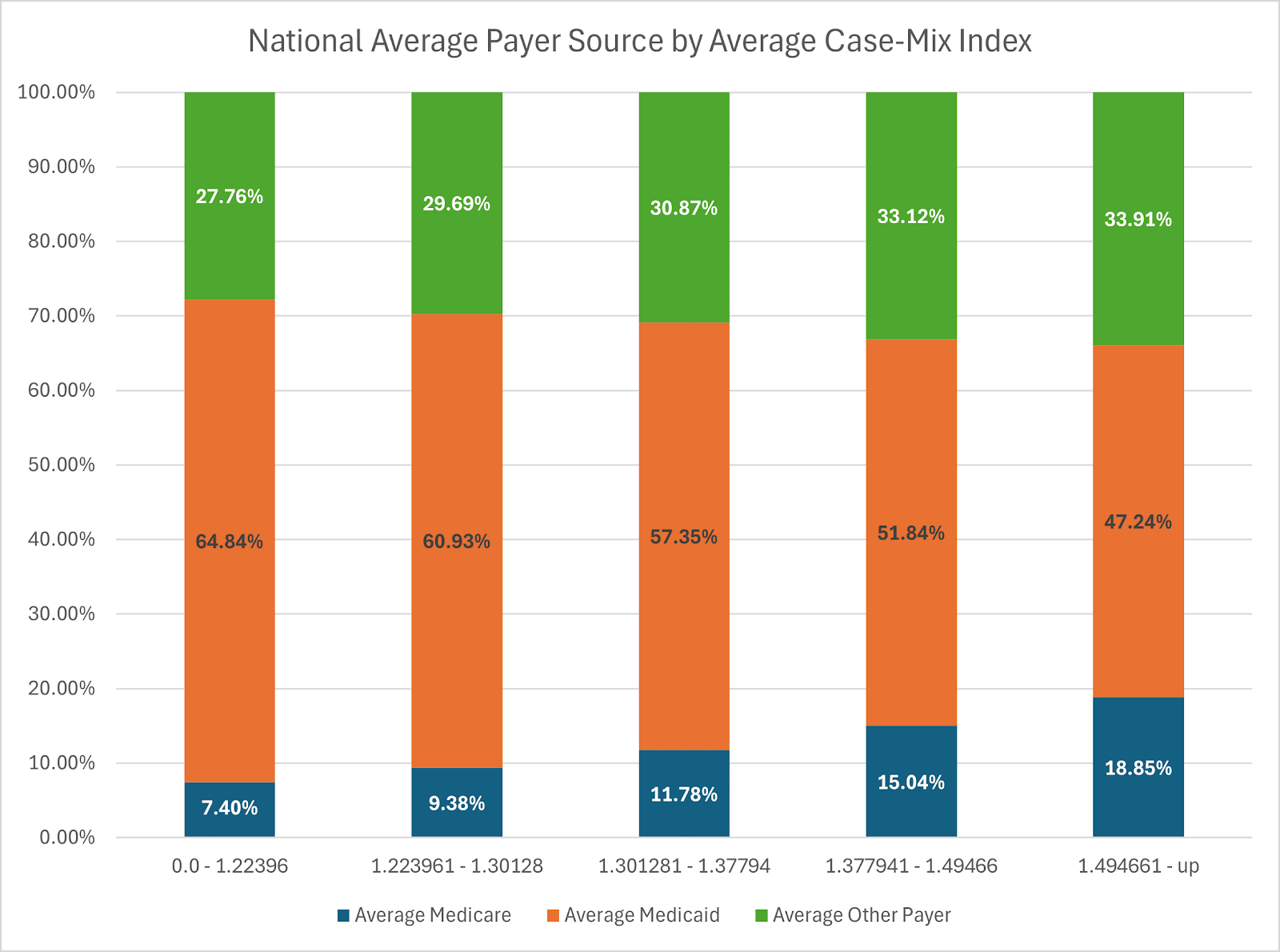
The chart above illustrates that a majority of facilities fall into the CMI range of 1.14 to 1.37, indicating that most nursing homes have residents with moderate care needs. However, this distribution can shift dramatically when looking at different payer sources, as we can see in the following table.
Facilities with lower CMI tend to rely more heavily on Medicaid, while those with higher CMI have a higher proportion of Medicare and other payers. This is significant because it suggests that payer mix directly impacts the CMI and, therefore, the staffing adjustments in Five-Star. That in and of itself isn’t necessarily noteworthy, but it invites a closer look at the impact of payment systems on Five-Star staffing adjustments.
The impact of state Medicaid reimbursement systems on nursing CMI
States that use a CMI-based Medicaid reimbursement system often see different CMI distributions compared to states that do not use this system. This creates a potential discrepancy in how nursing homes are evaluated under Five-Star.
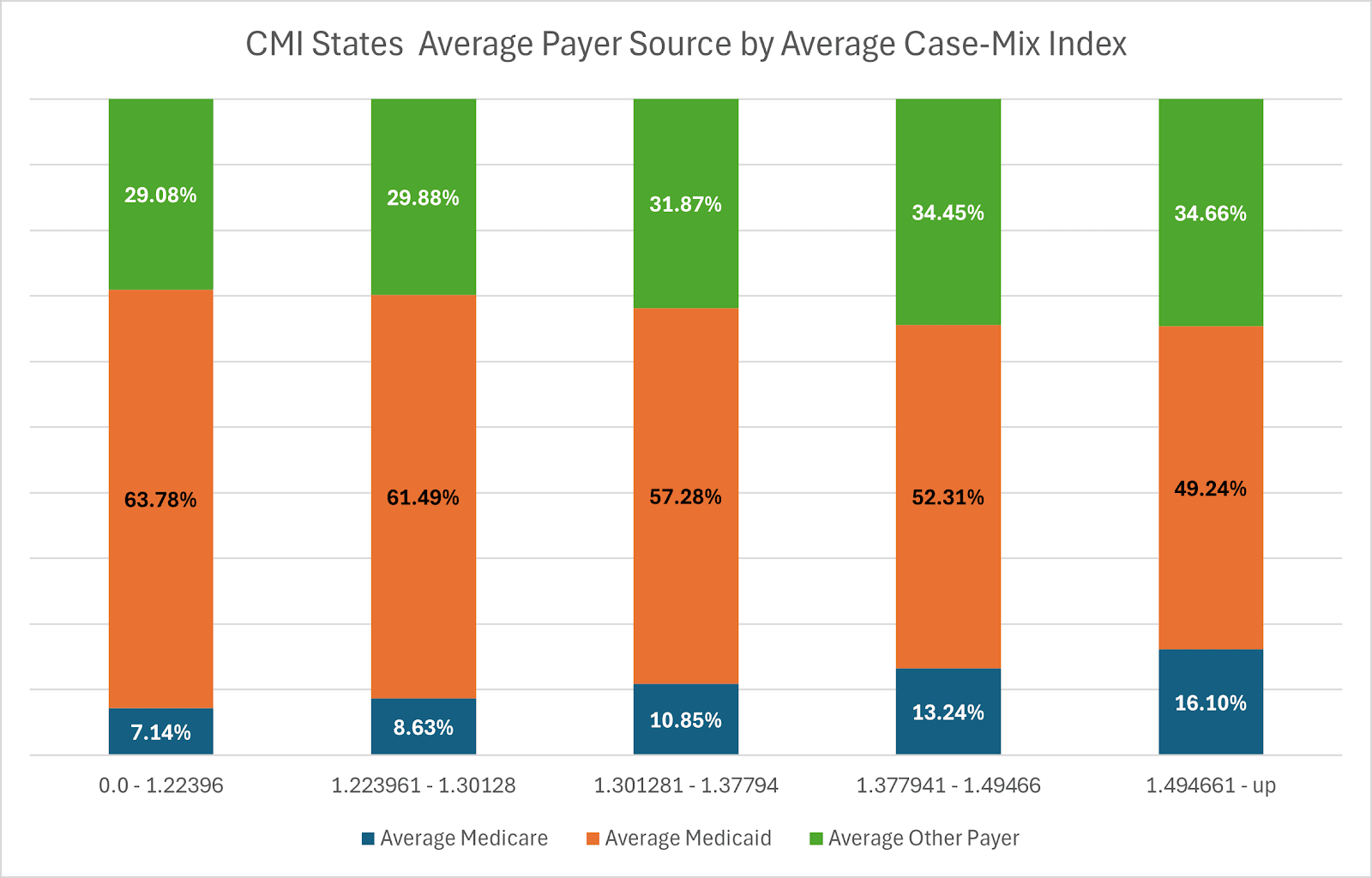
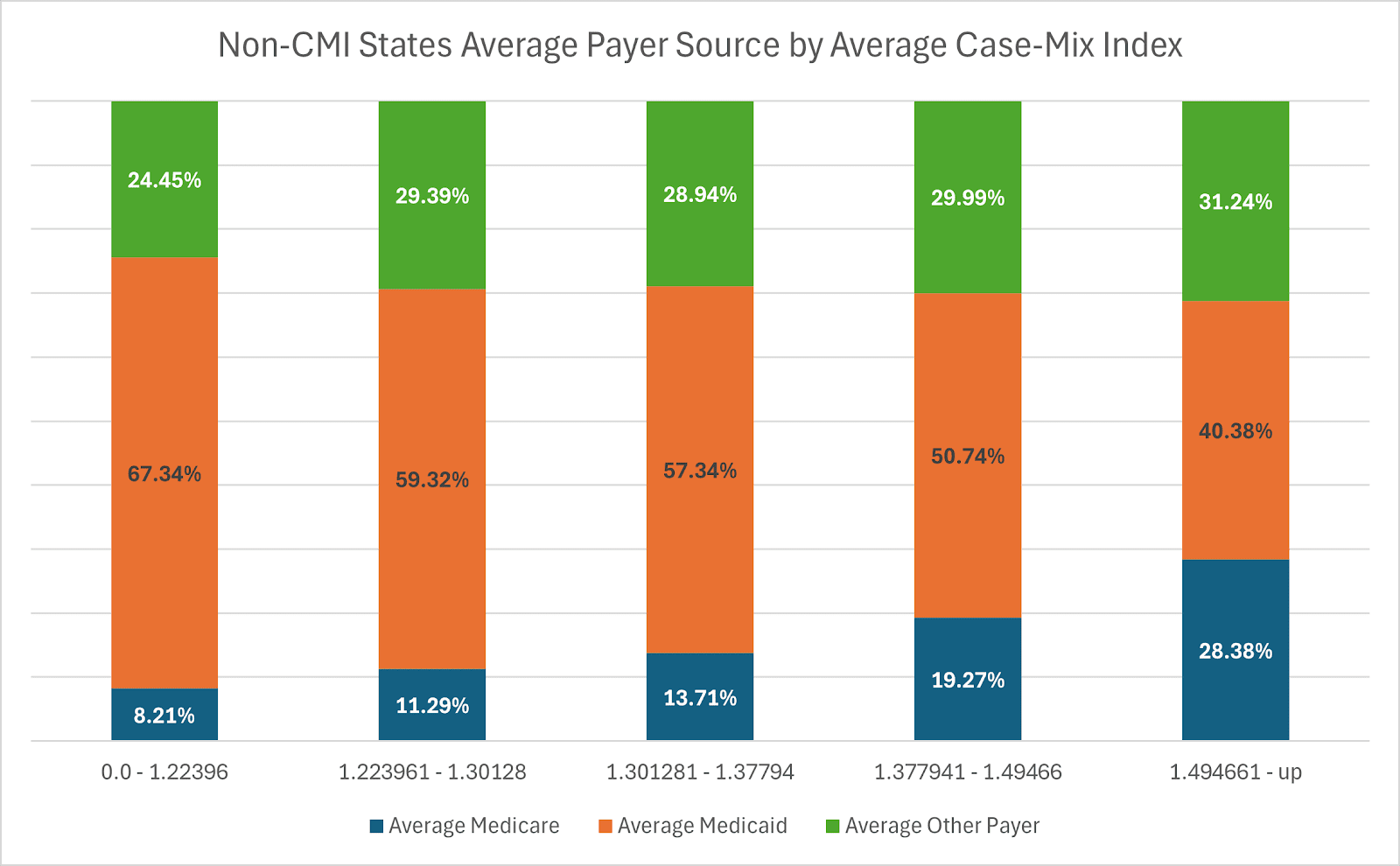
The charts reveal telling differences between CMI states and Non-CMI states. Simply put, CMI states have higher acuity Medicaid residents than non-CMI states.
The potential confusion
The way in which CMS adjusts Five-Star staffing ratings using nursing CMI may make it seem that facilities in CMI states are staffed at lower levels than those in non-CMI states. This adjustment, while intended to reflect resident acuity, may not fully account for the nuances of state Medicaid reimbursement systems. MDS coding directly impacts nursing CMI, and this coding differs between states that use it and states that do not. It distorts nursing homes’ actual performance, particularly in regard to staffing adequacy, and can thus be confusing for families and stakeholders.
CMS should reconsider its approach to staffing adjustments by moving away from using a national nursing CMI average. Instead, CMS should use state-level averages to accommodate local variations in coding and payment methodologies, much like the agency already does for health inspection (survey) outcomes. As CMS states in its Five-Star technical manual: “Medicaid pays for the largest proportion of long-term care in nursing homes. Nursing home eligibility rules, payment, and other policies in the state-administered Medicaid program may be associated with differences in survey outcomes.”
This same principle should apply to staffing adjustments. Just as state-specific benchmarks are used for survey outcomes to account for policy variations, CMS should apply a similar approach to nursing CMI adjustments, ensuring a more accurate and equitable reflection of nursing home performance across states.
Steven Littlehale is a gerontological clinical nurse specialist and chief innovation officer at Zimmet Healthcare Services Group.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.
Have a column idea? See our submission guidelines here.




